The Williamsburg Bridge is a suspension bridge that spans
Chapter 9, Problem 18SE(choose chapter or problem)
The Williamsburg Bridge is a suspension bridge that spans the East River, connecting the boroughs of Brooklyn and Manhattan in New York City. An assessment of the strengths of its cables is reported in the article “Estimating Strength of the Williamsburg Bridge Cables” (R. Perry, The American Statistician, 2002:211–217). Each suspension cable consists of 7696 wires. From one of the cables, wires were sampled from 128 points. These points came from four locations along the length of the cable (I, II, III, IV). At each location there were eight equally spaced points around the circumference of the cable (A, B, C, D, E, F, G, H). At each of the eight points, wires were sampled from four depths: (1) the external surface of the cable, (2) two inches deep, (3) four inches deep, and (4) seven inches deep (the cable is 9.625 inches in radius). Under assumptions made in the article, it is appropriate to consider this as a two-factor experiment with circumferential position and depth as the factors, and with location providing four replicates for each combination of these factors. The minimum breaking strength (in lbf) is presented in the following table for each of the 128 points.
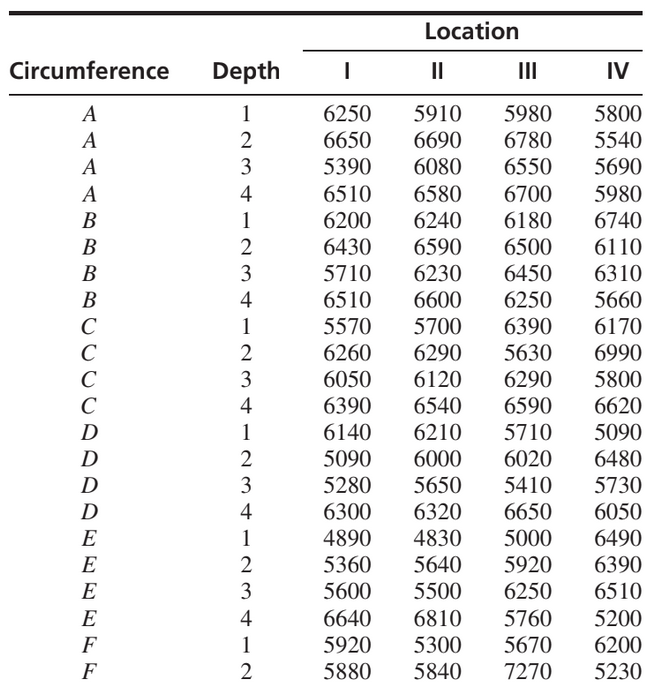
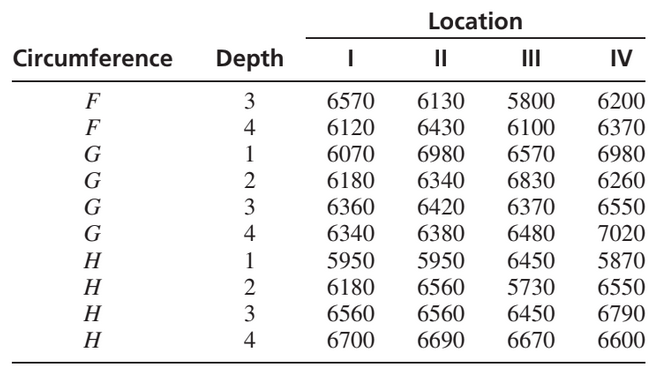
Construct an ANOVA table. You may give ranges for the P-values. Can you conclude that there are interactions between circumferential position and depth? Explain. Can you conclude that the strength varies with circumferential position? Explain. Can you conclude that the strength varies with depth? Explain.
Unfortunately, we don't have that question answered yet. But you can get it answered in just 5 hours by Logging in or Becoming a subscriber.
Becoming a subscriber
Or look for another answer